

For this review, I want to summarize the findings on the dietary carbohydrate to protein ratio and how it may influence body composition and blood lipid profiles in adult women.
There is evidence that older adults experience age-related changes in body composition, such as increase in body fat and decrease in lean body mass (Kim, O’Connor, Sands, Slebodnik, & Campbell, 2016). A moderate energy restricted diet is often an effective way for overweight adults to reduce bodyfat mass, and improve their health profile, but it often comes with the price of a loss of 25% of body mass being lost as lean body mass (Kim et al., 2016). Accumulating data suggests that increased protein content of the diet, in combination with exercise training, can reduce the loss of lean body mass in overweight and obese subjects following a weight loss diet. This preservation of lean body mass has been attributed to the increased level of essential amino acids, especially leucine, provided by the protein (Mettler, Mitchell, & Tipton, 2010).
Current dietary guidelines recommend a daily macro-nutrient intake of 55% carbohydrate, 30% protein and 15% fat (Layman et al., 2003). However, this balance has been challenged by evidence from epidemiological, clinical and experimental studies, reporting that a higher carbohydrate intake can reduce oxidation of body fat and increase blood triglycerides (Layman et al., 2003). In particular, the optimal ratio of carbohydrate to protein has been challenged on the basis of glucose homeostasis in the context of body mass reduction. Under a higher carbohydrate intake, the body has to rely on insulin to metabolize and dispose large quantities of dietary glucose, whereas under lower carbohydrate intakes (<200g per day), the body would rely more on hepatic production to maintain blood glucose via gluconeogenesis or glycogenolysis (Layman et al., 2003).
A study conducted in 2003 by Layman et al (2003), compared the results of a moderate protein and lower carbohydrate intake to a higher carbohydrate with lower protein intake, and the influence on body mass and blood lipids. In this study, the total energy intake, fat and fiber were consistent among the two groups: 1700 kcal/day, total fat intake was 50g/day and total fiber at 20g per day. In the higher protein group (Protein Group) protein intake averaged 125g/day with a carbohydrate intake of 171g/day. The higher carbohydrate group (CHO) consisted of 68g pf protein per day and 239g of carbohydrates. The relative proportions of energy in the Protein Group were 30% protein, 41% carbohydrate and 29% fat with a ratio of carbohydrate to protein (CHO/protein) of 1.4. The proportion in the CHO Group was 16% protein, 58% carbohydrate and 26% fat with a ratio of 3.5 (Layman et al., 2003). Obviously, the cholesterol and saturated fatty acid intake was higher in the Protein group than the CHO group.
The study duration was 10 weeks. The results of the study indicated the following:
- There was not a big change in body weight between the two groups. The Protein Group lost a total weight of 7.53kg and the CHO group lost 6.96kg.
- Changes in body composition indicate the weight loss was mostly bodyfat. The Protein group lost 14.4% of initial body fat, the CHO group lost 12.2% of initial bodyfat. Loss of lean body mass tended to be greater in the CHO Group compared to the Protein Group. When changes in body composition were expressed as a ratio of fat/lean loss, the Protein group achieved a fat/lean loss of 6.36 vs. 3.92 in the CHO group. The higher protein group clearly had a stronger improvement in body composition.
- There were some differences seen in thyroid hormones, blood lipids and fasting and postprandial glucose and insulin levels, but it was not explained in detail as it was not the main objective of this study.
In summary, the results of this study indicate that the positive changes in body composition associated with the higher protein diet may be associated with either targeting of body fat or sparing of muscle protein, or both. For the purposes of improving body composition, a higher protein diet may be effective for adults.
Before I end this summary, I do want to mention I did stumble upon an interesting study in 2016 that indicates that a high protein intake eliminates the weight loss induced improvement of insulin action on postmenopausal women (Smith et al., 2016). This study indicates that a high protein diet can have adverse effects on postprandial insulin sensitivity. According to the authors, “the beneficial effect of 10% weight loss on muscle insulin action (assessed as glucose disposal rate and phosphorylation of AKT in muscle during a HECP) was eliminated by high protein (HP) intake” (Smith et al., 2016). The failure to improve muscle insulin sensitivity in the higher protein group is clinically important, because it reflects a failure to improve a major mechanism involved in the development of T2D. It also indicates more insulin is required in the higher protein group to dispose of a given amount of glucose. This can be due to:
- BCAA’s, particularly leucine, that can impair insulin mediated uptake of glucose through a negative feedback inhibition
- There may be an association of glycine and tryptophan and metabolites of acylcarnitine in the development of insulin resistance, regardless of the amount of circulating amino acid metabolites measured in the serum.
- There may be a metabolic process related to oxidative stress that is expressed in the higher protein group, as evidenced by gene expression of GSTA4 and PRDX3 that are both associated with oxidative stress. These results suggest that the adverse effect of high protein intake on insulin action during weight loss therapy may have been mediated through its effects on oxidative stress because it prevented the WL-induced decrease, and even increased, metabolic pathways involved in oxidative stress response in muscle.
- Both groups had improved liver insulin sensitivity, but the higher protein group experienced a reduction in muscle insulin sensitivity. This is attributed to the fact that protein is a potent insulin secretagogue, which may overcome the adverse effect of protein on insulin sensitivity by increasing the secretion of insulin (Smith et al., 2016).
I must mention however, protein causes greater satiation and has a greater thermogenic effect of feeding than carbohydrate and fat. This alone can lead to greater weight loss with a higher protein than a standard protein diet. “Therefore, the adverse effect of dietary protein on muscle insulin action could be offset by its effect on hepatic insulin sensitivity, insulin secretion and energy balance” (Smith et al., 2016).
In summary, this review demonstrates that the protein content of a weight loss diet can have significant effects on metabolic function and weight loss outcome. I personally believe that diets should be personalized for the individual. A high protein diet is not suitable for everyone. Neither is a high carbohydrate diet. The individual’s needs should be taken into consideration, along with various markers of health that can be measured in a blood chemistry panel, their nutritional needs (such as macronutrient deficiencies) and even nutrigenomics, health predispositions and family history. The one size fits all approach is not appropriate when prescribing nutrition therapy, as the results of these studies also demonstrate.
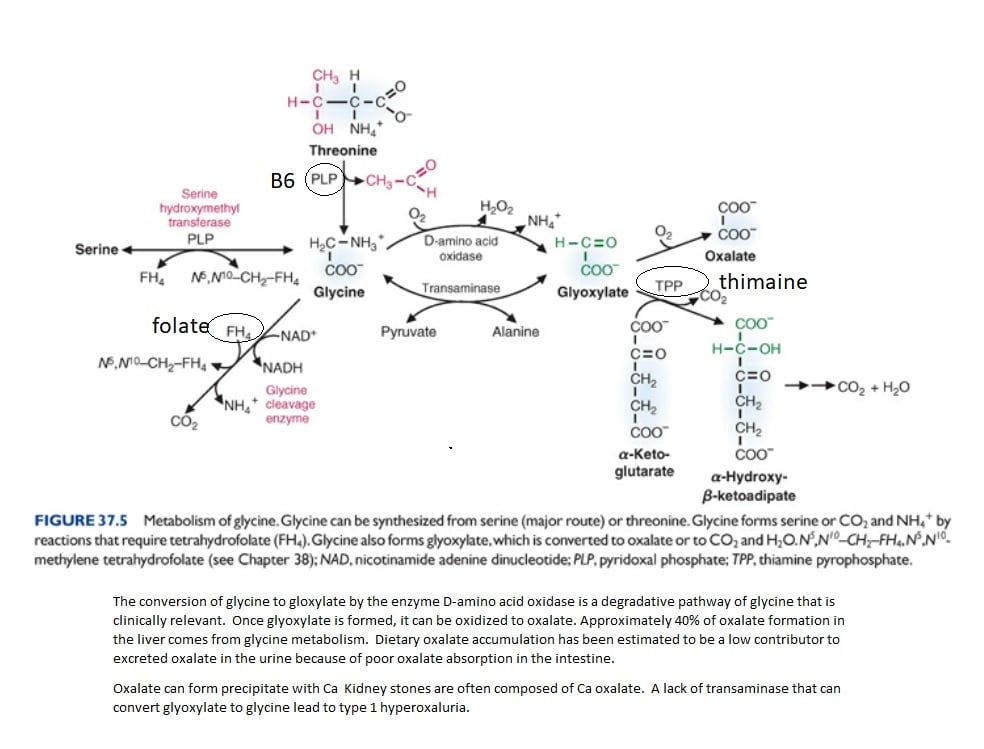
What do I think? The evidence is good for a higher protein diet, but I wonder if they looked into the glucogenic amino acids and their effect on insulin sensitivity. In my review, I found another journal that indeed indicated that various amino acids can actually decrease insulin sensitivity. Interestingly, it was leucine that was contributing to this change in muscle insulin sensitivity, and that is actually a ketogenic amino acid! If I find the free time at some point, I would love to research the effects of glucogenic and ketogenic amino acids and how they affect insulin sensitivity and type 2 diabetes. I personally have not been a fan of high protein diets. I feel it is too hard on the kidneys, and considering glycine is often a problem with oxalate metabolism, especially in the context B1 deficiency, I feel the risk of kidney stones is too great to recommend high protein across the board (See image). I prefer a more balance approach, with a balance of macronutrients and incorporating intermittent fasting as a way to improve blood lipids and insulin sensitivity.
References
Kim, J. E., O’Connor, L. E., Sands, L. P., Slebodnik, M. B., & Campbell, W. W. (2016). Effects of dietary protein intake on body composition changes after weight loss in older adults: a systematic review and meta-analysis. Nutr Rev, 74(3), 210-224. doi:10.1093/nutrit/nuv065
Layman, D. K., Boileau, R. A., Erickson, D. J., Painter, J. E., Shiue, H., Sather, C., & Christou, D. D. (2003). A Reduced Ratio of Dietary Carbohydrate to Protein Improves Body Composition and Blood Lipid Profiles during Weight Loss in Adult Women. J Nutr, 133(2), 411-417. doi:10.1093/jn/133.2.411
Mettler, S., Mitchell, N., & Tipton, K. D. (2010). Increased protein intake reduces lean body mass loss during weight loss in athletes. Med Sci Sports Exerc, 42(2), 326-337. doi:10.1249/MSS.0b013e3181b2ef8e
Smith, G. I., Yoshino, J., Kelly, S. C., Reeds, D. N., Okunade, A., Patterson, B. W., . . . Mittendorfer, B. (2016). High-Protein Intake during Weight Loss Therapy Eliminates the Weight-Loss-Induced Improvement in Insulin Action in Obese Postmenopausal Women. Cell Rep, 17(3), 849-861. doi:10.1016/j.celrep.2016.09.047


")